How SLPs can move towards a neurodiversity affirming approach
SLPs are moving away from ableist models and towards neurodiveristy-affirming approaches, but what does that look like? Here, I reflect on changes that neurodiversity advocates have promoted, and why that is central to evidence-based practice.
NEURODIVERSITY-AFFIRMING PRACTICE
Katie Abendroth
6/1/20255 min read


What is neurodiversity affirming speech and language?
Speech-language pathology (SLP) social media feeds are filled with neurodiversity tips and buzzwords. But what does a neurodiversity-affirming approach to speech and language therapy really look like?
The biggest professional change that I have made is moving away from deficit models. That’s a big change since I was in graduate school for speech-language pathology. The terms, diagnostic categories, and goals have all shifted towards supporting neurodiversity and away from a disability model and towards a social model of disability.
Masking goals can take many different forms, but have the common theme of pushing a client to exhibit “more neurotypical” behaviors. A masking goal for a stutterer may include fluency measures, while a masking goal for Autism may target less compensatory strategies or “stimming.” For a child with Tourette syndrome, a masking goal may target fewer tics.
Masking goals are problematic because research shows they cause tremendous stress to the neurodiverse client. They require cognitive effort and energy that is distracting and takes away from learning. You can read more here.
What can we do instead? First, it is important to be able to change our own language. Speech-language assessment and treatment models are increasingly moving away from deficits-based instruction, which can lead to challenging conversations with both families and insurance companies.
Below are changes that I have adopted in actual speech and language practice, and I hope you will too. You will find them in my products, posts, and client goals.
1. Autism (Removing “Spectrum Disorder”)
I have tried to remove the phrase spectrum disorder from my posts, products, and resources. If you catch one in a product description, please drop me a line! I am making an effort to respond to the autism community by modifying this language.
Although autism and ASD are often used interchangeably, the World Health Organization (WHO) explains more here.
Why remove the word “spectrum” from autism spectrum disorders? There has been a lot of change in the use of the word “spectrum” as it pertains to autism. The concept of spectrum implies that there is a point where neurodivergence blends into neurotypical populations.
The problem is that embracing spectrum, according to neurodiversity proponents, is that it leads to a false narrative that everyone is “a little” Autistic, or “a little” ADHD. It dilutes the value of this label.
Why remove the word “disorder” from autism spectrum disorders? To endorse a neurodiversity-affirming approach and to promote inclusion, professionals should carefully consider the word “disorder” and whether it has any place in our practice as speech-language pathologists.
Moving towards a social model and away from a medical or deficit model takes ongoing advocacy.
2. Autism (with a capital A)
A second change I made in my products, posts, and wording is writing Autism with a capital A. This refers to the community and culture of a distinct group. Again, the advocacy community shows a growing preference for using Autism with a capital A, as described here, to convey community and inclusion.
Of course, not everybody feels this way and “autism” is a heterogenous category. It encompasses many different perspectives and individuals.
SLPs and educators should remember that for parents, this may be a club they never imagined being part of, and it takes time to grieve and accept their child for the unique individual they are.
3. Identity-first language
As explained here, advocates have promoted identity-first language. Preferred terms include Autistic or Autistic person, but often parents and professionals challenge this wording.
In full transparency, this change still feels unnatural to me because of how heavily “person-first language” (e.g., person with Autism) was emphasized when I was a graduate student in speech-language pathology. In the early 2000’s, professionals were taught that person-first language in healthcare was a sign of respect and recognition that the patient in front of you is human first.
However, many Autistic individuals are comfortable with using Autistic as a community label and refrain from using the phrase “person with autism.”
Similarly, a department in our local university changed their name from the “Students With Disabilities Access Center,” to “Disability Access Services,” reflecting identity-first language.
The other day I used “Stutterer” rather than “person who stutters.” This honestly is a learning curve for me, but I am trying to implement that norm as it is preferred among advocates. Ultimately, people should be allowed to self-identify and for older clients, SLPs should ask them how they want to be described.
I would love to hear your feedback on this one, email me at info@ddvspeech.com if you work in schools or healthcare settings.
4. Celebrate Red
If you have worked in the Autism community long enough you remember when blue was promoted during the month of April as a way to celebrate autism awareness and acceptance. Now people prefer the #WearRedInstead hashtag, which aligns with self advocacy.
The color blue was first promoted by Cure Autism Now which, as a group has presented controversial stances related to a cure for autism. Using red instead refutes this agenda and the medical model of disability at its foundation.
5. Writing neurodiversity-affirming goals and accommodations
As I mentioned in a previous article, and above, goals and accommodations should not focus on changing the individual on your caseload to be “more typical.” Neurodiversity-affirming goals and accommodations have a few things in common:
First, goals put equal focus on educating your client and their peers or family. The double empathy problem reveals how neurotypicals also need education to facilitate understanding. Read Autism and the double empathy problem: Implications for development and mental health (Mitchell, Sheppard, & Cassidy, 2021) to learn more.
Second, self-advocacy is a core component. Whether that means the client you work with learns to say no, ask for a break, or create a video about their learning style, the focus is on support.
Third, neurodiversity-affirming goals are client centered. The client drives what they want to improve, learn, or target. If your client does not use words to speak, an augmentative and alternative communication (AAC) system may be the starting point to accessibility.
If your student stutters and wants to learn fluency strategies that they can choose to use, that can be part of their speech-language goal.
Neurodiversity is a concept that continues to evolve. It is helpful to keep collaborating with your clients and other SLPs to find the best solutions within your setting. If you work with families directly, there may be a family education or counseling component that needs to happen.
Do you have challenges with incorporating neurodiversity-affirming approaches with your older speech therapy students? Drop me a line at info@ddvspeech.com or DM me on IG @ddvspeech and I would love to connect.
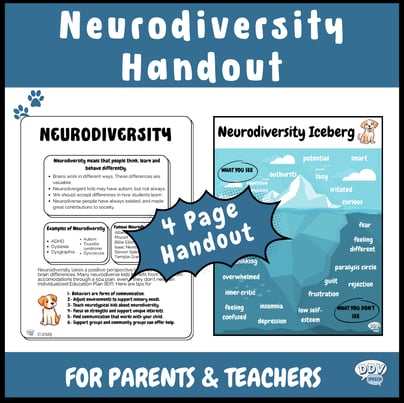
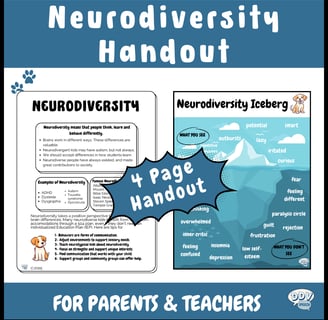
Before you go, grab your free neurodiversity handouts!
When you join my community, I will send a monthly freebie to use with your middle school speech and language students.
Resources
Join my pack and get started with free neurodiversity-affirming handouts for speech-language pathologists.
contact
Connect
© 2024. All rights reserved.